Operational Manual
Know the terrain before you move.
The operational manual covers the non-clinical fundamentals of retrieval practice — the geography, the workplace, the team, and the standards that govern how we operate.
Operational Theatre
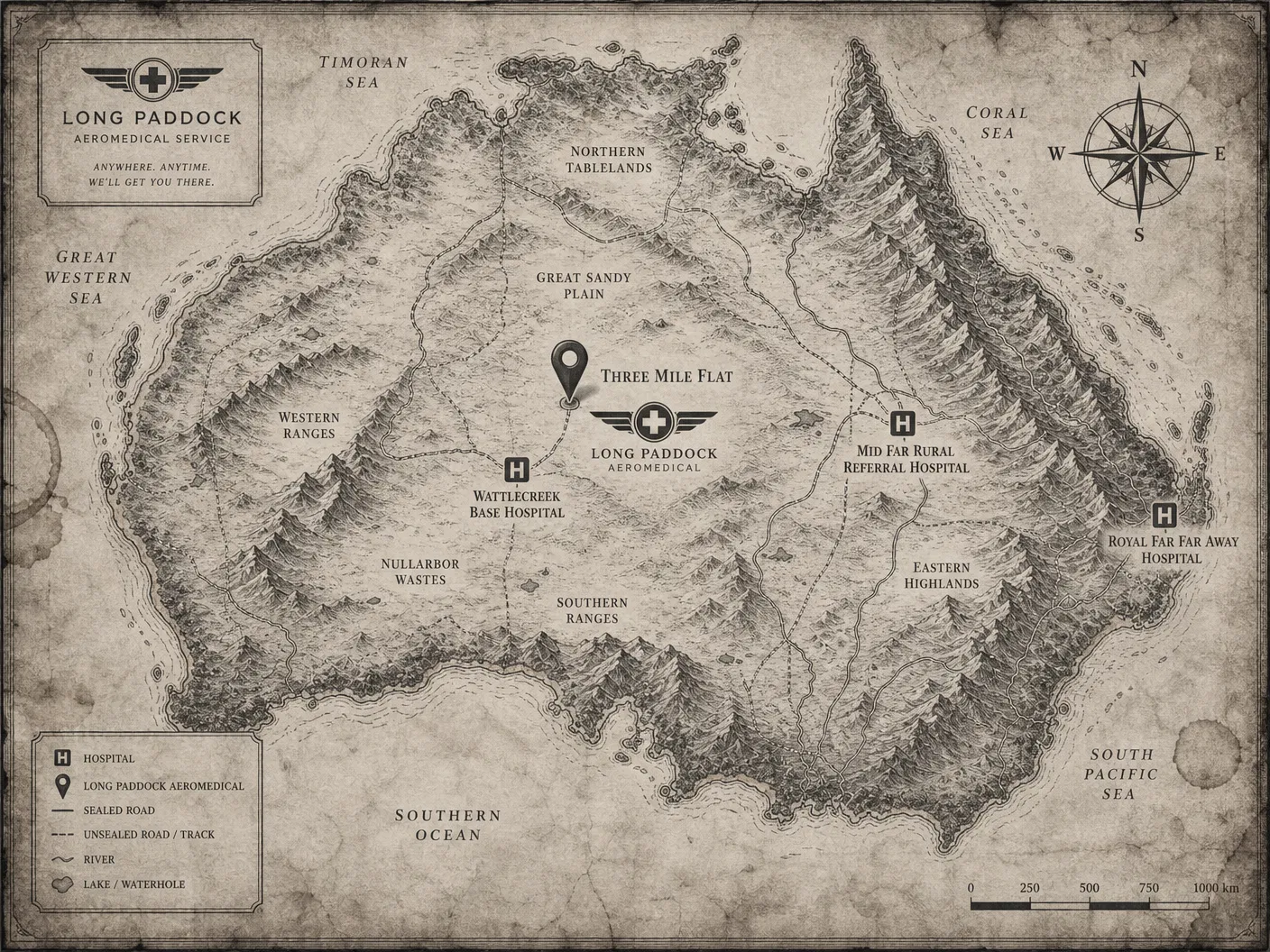
Where we work.
Retrieval medicine does not happen in a single place. It happens in the space between places — in the aircraft, on the road, at the edge of what a local service can manage. Understanding your geography is the first step to understanding your risk.
Operational realities at Long Paddock Aeromedical
A working note for new crew, written in the spirit of "you will figure this out the hard way unless we tell you first."
Clause 1 — Operational Footprint
The Long Paddock retrieval network spans metropolitan, regional, and remote settings across most of the country, plus a few places that haven't quite decided whether they belong to the country or to themselves. Our operating environment varies dramatically by geography — from urban trauma scenes (where the hospital is fifteen minutes away and the parking is the problem) to regional centres (where the hospital is four hours away and the parking is also the problem) to remote pastoral properties (where the hospital is a concept), offshore platforms (where the hospital is a helicopter pad and a freezer), and island communities (where the hospital is whoever happens to have done a first aid course in the last decade and is willing to admit it).
Each zone carries its own risk profile, its own logistics constraints, and its own special category of resource limitation. Mags has worked in all of them. Mags has opinions about all of them. You will hear most of these opinions in due course, often in response to questions you didn't ask, occasionally in response to questions you didn't realise you'd asked but which Mags inferred from the look on your face.
Clause 2 — Environmental Hazards
Altitude, temperature, terrain, and weather are not background conditions. They are active clinical variables, and they will conspire against you the moment you stop respecting them.
A patient who is stable at sea level may deteriorate rapidly at 8,000 feet, which is the altitude at which the cabin is pressurised to despite Davo's best efforts to fly lower. A team that is effective in temperate conditions may face significant capability degradation in a wet-season tropical environment, where the humidity is 94%, the patient's drips are condensing inside the giving sets, and Toby has discovered that his glasses don't work above 32 degrees. A clinician who has done a thousand RSIs in the resus bay may discover, at altitude, in turbulence, with a patient whose neck is shorter than they noticed at sea level, that retrieval medicine is its own sport.
Know your zone before you commit. The phrase "I've done this before" applies at sea level. It applies less well at altitude. It applies not at all in the back of a road ambulance on a corrugated track at 2am, which is its own ecosystem and has produced its own lessons, most of them learned by people who are now extremely cautious about corrugated tracks.
Clause 3 — Living Hazards
The country we operate in contains, in addition to the patient, a wide variety of biological entities that would prefer the patient remain where they are.
Snakes. The strip you have just landed on may be home to one of approximately fourteen species that you would rather not meet, three of which can kill you in under two hours and one of which is so well-camouflaged that Stretch has stepped on the same individual twice in different decades. Look before you walk. Walk before you run. Do not run unless Stretch is also running, in which case sprint without asking why. Bishop carries pressure bandages in three places on her person at all times for reasons she will not discuss.
Spiders. The aircraft that has been parked in the hangar for six hours has been parked there with the doors open. Mathematics will tell you what has happened in those six hours. Check the cabin before loading. Check the stretcher before loading. Check the patient if the patient has been waiting near the strip. Toby once loaded a patient who arrived with a hitchhiker and we do not speak of what followed, although Bishop wrote a field note about it that is required reading.
Crocodiles. If your tasking takes you north of a certain line, the rules change. The patient on the riverbank, the strip near the billabong, the thoughtful walk to stretch your legs while the aircraft refuels — all of these are in a different category of decision than they would be elsewhere. The local rule is that anything that looks like a log is not a log, and anything that looks like it might not be a log is definitely not a log. Do not approach water. Do not turn your back on water. Do not assume that water you cannot see is not water that can see you. Davo has lost a flying suit to this principle and will not be drawn on the details.
Cattle, on a strip. Common. Persistent. Not actively hostile but not in any hurry to relocate. Approach via low pass to encourage relocation. If unmoved, contact the station owner via the number provided in the tasking pack. If no station owner is available, Davo will have a view, and the view will be expressed using the aircraft.
Wildlife generally, on a strip. Various. Unpredictable. The strip that was clear on approach may not be clear on touchdown. The flock that scattered at the noise of the engine has not necessarily scattered permanently. Do not relax until you have rolled to a stop and the windsock is the only thing moving.
Mosquitoes, in the wet. Will not kill you tonight. Will give you something interesting to read about in three weeks. Use the repellent Stretch issues from the supply cupboard, which smells like industrial degreaser because, technically, it is.
The patient's family dog. Often a working dog. Sometimes deeply protective of the patient. Bishop has techniques. Toby has scars.
Clause 4 — Landing Sites & Access
Landing site assessment is a core retrieval competency. It is also the part of the job where the medical team most needs to sit down, drink water, and let the pilots think — the airway, the haemodynamics, and the blood gas can wait three minutes. The runway cannot.
Evaluate surface, slope, obstacles, last light, and alternate options before accepting a tasking. The strip that looks acceptable on the satellite imagery may, on closer inspection, contain three head of cattle, a windsock pointing in a direction not previously contemplated by the meteorological office, several small animals who consider the runway their personal property, the aforementioned crocodile that is definitely not a log, and a tractor that the property owner swears was moved last week. Satellite imagery is from last summer. The strip is from this morning. They are not the same strip.
Surface. Bitumen is a luxury. Compacted dirt is the norm. Wet compacted dirt is a different proposition entirely and has been the subject of three field notes, two incident reports, and one quiet conversation between Mags and a junior pilot that ended that pilot's career trajectory. If the strip looks like chocolate icing, it is chocolate icing. Do not commit.
Slope. Strips are rarely flat. The strip that appears flat from above may have a 4% gradient that you only notice when you're rolling out and the brakes are working harder than they should be. Davo has a phrase for the moment of realisation, which is unprintable.
Obstacles. Powerlines are the great underestimated hazard. They do not show up on satellite imagery. They are sometimes not on the strip diagram. They are always there. Look for the poles, infer the lines, assume the worst. The fence the property owner described as "removed" may have been mentally removed but not physically removed.
Last light. Last light is real. Last light does not negotiate. Last light has ended more retrievals than weather, mechanical failure, and clinical deterioration combined. The clinical urgency that justified departing at 4pm does not justify arriving back at 7:32pm in an aircraft rated for VFR operations only. Davo will not fly into night VFR. Davo has not flown into night VFR in twenty-two years and is not starting tonight. The patient will be fine. The patient was, statistically, going to be fine before the call came in. Last light is non-negotiable.
Alternates. Have one. Brief one. Know its surface, its length, its hazards, and its distance from definitive care. The number of crews who have committed to a strip with no alternate, encountered the unexpected on arrival, and discovered that the unexpected has no plan B is non-zero. We would prefer the number remain non-zero rather than become larger.
A retrievable patient who cannot be extracted safely is not a retrieval. It is, in Davo's preferred phrasing, "a body recovery problem with extra steps." This is a piece of operational wisdom that should be tattooed on every junior retrievalist's forearm, but isn't, because Bishop has views about tattoos and the subject is not currently open for discussion.
When in doubt, do not commit to the strip. The hospital that doesn't get the patient tonight will get the patient tomorrow. The strip that takes the aircraft will not return it. Mags has been on three retrievals where the strip was the right answer and one where it wasn't. The one where it wasn't is the one she still talks about, occasionally, in the crew room, when the conversation has gone quiet and somebody is about to make a decision they shouldn't.
Clause 5 — Communication Dead Zones
Assume comms will fail at the worst possible time. This is not pessimism. This is the lived experience of every retrieval crew that has ever existed, codified into a working principle by Stretch, who has personally watched seven different communication systems fail in seven different ways at seven different moments when they were most needed. Stretch keeps a tally. The tally is now in double figures and Stretch has stopped updating it for legal reasons.
Know your backup plan before you depart. The hierarchy of redundancy at Long Paddock is, in order of reliability:
HF radio. Works when the conditions are right. Conditions are rarely right. When conditions are right, HF will reach you from the other side of the continent. When conditions are wrong, HF will not reach the next paddock. The only person who reliably understands the conditions is Stretch, who consults what appears to be a homemade chart and refuses to share his methodology.
Satellite phone. Works when it has signal, charge, and is not currently in the kitchen at base where Toby left it. The satellite phone has been left in the kitchen four times. Each time has been documented. Each time, Toby has agreed to a system to prevent it happening again. Each time, the system has failed.
Mobile phone. Works when you are within coverage, which is to say not when you need it. Coverage maps are aspirational documents. The coverage you experienced on the way out is not the coverage you will experience on the way back, because coverage moves. We do not know why coverage moves. We assume it has its reasons.
EPIRB relay. Works once, briefly, decisively. If you are using the EPIRB you are not using anything else, and a number of people are about to have a busy afternoon. Do not test the EPIRB. The last person to test the EPIRB resulted in three coast guard call-outs and a phone call from Canberra that Mags had to take. Mags has not yet recovered.
The handheld radio Stretch insists on issuing. Has saved Toby three times. Toby still describes it as "probably overkill." Stretch and Toby are not currently in agreement on this point and the matter is considered open.
The cattle station owner's landline. The most reliable communications technology in existence. Has not failed in forty years. The phone number is in the tasking pack. The tasking pack is in the cabin. Read the tasking pack before you depart. Read the tasking pack again before you land. The number for Mrs Henderson's homestead (no relation to Davo, although there is a story there) has resolved more comms failures than every electronic system combined.
Stretch's pigeons. Stretch denies maintaining pigeons for emergency comms. The aviary behind the hangar is, according to Stretch, "for personal reasons." The aviary has been there for nineteen years and the pigeons have been there for nine of them. Make of this what you will.
Do not rely on a single communications pathway for a time-critical transfer. Do not assume the mobile coverage that worked on the way out will work on the way back. Do not assume the satellite phone that was charged on Tuesday is still charged on Friday. Do not assume the dispatcher heard your last transmission until they confirm they heard your last transmission. The phrase "they probably got it" has preceded more incident reports than any other in the history of the service. The runner-up is "I'm sure it's fine." The bronze medal goes to "what could possibly go wrong," which is the phrase Mags has banned from the crew room and which Toby continues to use anyway.
If your comms fail entirely, the agreed protocol is to make the safest clinical decision you can with the information you have, document everything, get the patient to a place where comms exist, and then explain yourself to Mags, who will listen patiently to the entire account before asking the one question you should have asked yourself an hour earlier. Mags has been asking that question for twenty years. The question is always the right question. The question is never the question you wanted.